Case Report
Bouveret Syndrome in an Elderly Female

Zvi H. Perry1,2*, Udit Gibor1, Shahar Atias1, Solly Mizrahi1, Alex Rosental1 and Boris Kirshtein1
1Department of Surgery A, Soroka University Medical Center, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel
2Moshe Prywes Center for Medical Education, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel
3Department of Gastroenterology, Soroka University Medical Center, Ben Gurion University of the Negev, Beer-Sheva, Israel
*Address for Correspondence: Zvi Perry, MD, Department of Surgery A, Soroka University Medical Center, PO Box 151, Beer-Sheva 64101, Israel, Tel: +972-8-640-0610, +972-50-340-0902; Fax: +972-8-647-7633; Email: [email protected]
Dates: Submitted: 26 December 2016; Approved: 28 December 2016; Published: 03 January 2017
How to cite this article: Perry ZH, Gibor U, Atias S, Mizrahi S, Rosental A, et al. Bouveret Syndrome in an Elderly Female. Arch Surg Clin Res. 2017; 1: 012-015. DOI: 10.29328/journal.ascr.1001002
Copyright License: © 2017 Perry ZH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Introduction: A gastric outlet obstruction secondary to a gallstone ileus is known as Bouveret syndrome. Herein we present a case of an elderly woman with an impacted gallstone in duodenum and discuss its’ management.
Patient description: A 96-year-old woman was admitted to our department due to a gastric outlet obstruction. Initial gastroscopy revealed a gastric bezoar. An attempt for its extraction failed. She underwent a laparotomy in which a cholecystoduodenal fistula and a large impacted stone were found. Separation of the fistula, including closure of the duodenum side, cholecystectomy and removal of the obstructing gallstone were performed. Additional stones were found and retrieved during common bile duct (CBD) exploration. Surgery was finalized by duodenoplasty, closure and T-tube drainage of the CBD. Post-operative course was prolonged and uneventful.
Discussion and Conclusions: Bouveret syndrome is a rare cause of gastric outlet obstructions. In this case, unsuccessful endoscopic treatment necessitated surgery for removal of impacted gallstone in the duodenum.
INTRODUCTION
In the general population Gallstone ileus accounts for 1%-3% of small bowel obstructions. The majority of obstructing gallstones are located in the terminal ileum [1]. Less than 10% of impacted gallstones are located in the duodenum [2]. It is reported that 80% of the time, enteric gallstones pass spontaneously [3]. A gastric outlet obstruction secondary to a gallstone ileus is known as Bouveret syndrome [4]. There is a 5:1 female to male predominance reported, with elderly women in their sixth or seventh decade of life most commonly affected [5]. Obstruction occurs more often with gallstones greater than 2.5 cm in diameter [6].
We report a case of a patient with Bouveret syndrome and discuss it’s management.
CASE PRESENTATION
A 96-year-old female had been admitted due to abdominal pain and coffee ground vomiting. A week previously she had been discharged from the Internal Medicine Department with a diagnosis of gastric bezoar that was found on gastroscopy and successfully extracted. Her medical history included chronic renal failure, hypertension, and diabetes, which were under control with subsequent medications. She was known to have biliary stones for 2 years, and it was decided not to operate upon her, due to advanced age and her medical condition. Upon admission her physical examination was unremarkable except for minor epigastric tenderness and faint bowel sounds. Her blood pressure was 157/51 mmHg, pulse 74 beats per minute, and body temperature 37.1ºC. A large amount of “coffee ground” content was drained after NG tube insertion.
Abdominal plain film revealed distended stomach and a large oval shadow in the distal part of the stomach with advancement of gastrograffin t around the oval shadow, into the rest of small bowel (Figure 1).
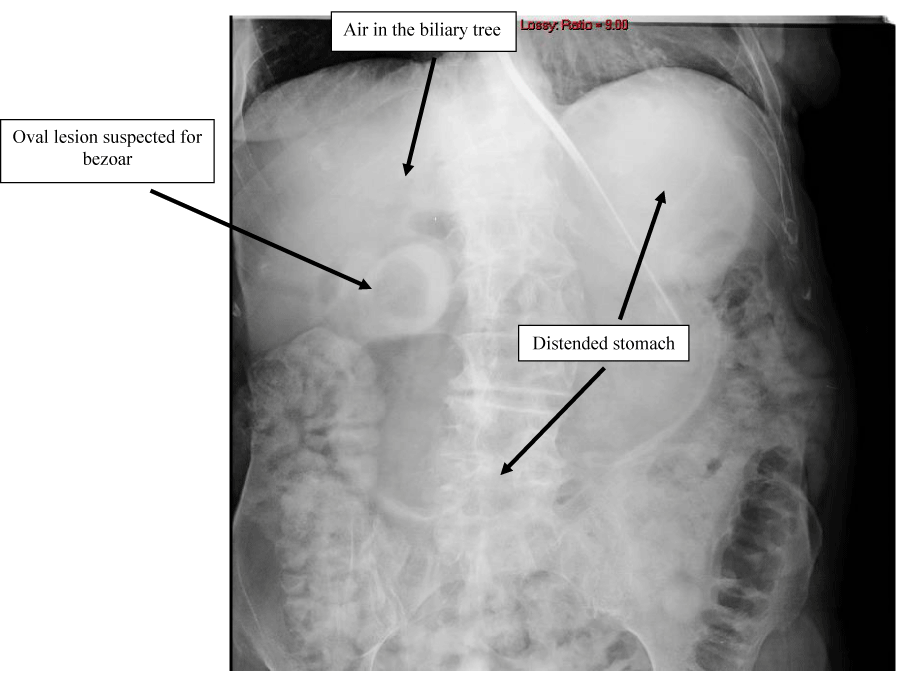
Figure 1: An abdominal plain film 3 hours after gastrograffin injection through NG tube upon admission.
IV fluids were started. Blood tests revealed a mild elevation of creatinine (1.4 mg/dL), anemia (Hb 9.8g/dL), and no leukocytosis (WBC 7.4×103µL).
Gastroscopy was attempted four times. During the last session partial extraction of bezoar was performed. However, it was unable to relieve the obstruction, and thus she was scheduled for surgery. A mid-line laparotomy was performed; a large lesion in the 4th part of the duodenum was palpated and a fistula between the gallbladder and the 2nd part of the duodenum was found.
The fistula had been resected and the gallbladder was removed; the gallstone in the duodenum was retrieved through the duodenal opening Figure 2. Exploration revealed another stone that had been removed through a choledochotomy. The final steps of the operation were closure of the CBD on a T-tube and a duodenoplasty. T-tube cholangiography two weeks post-operatively showed an intact CBD and the t-tube was removed. She was discharged three weeks after admission. Pathology results showed chronic cholecystitis and bile granulomata.

Figure 2: An extracted gallstone scaling with 10 cc syringe.
DISCUSSION
The literature concerning bowel obstruction due to gallstones, mainly those impacted in the duodenum, is scarce [1,4-6]. Patients may present with clinical symptoms of small bowel obstruction including nausea, vomiting, obstipation, and abdominal pain for a few days. Bilious vomiting is characteristic of a proximal obstruction, whereas feculent vomiting and abdominal distension are more commonly seen in more distal obstructions.
In the current presentation we described a 96-year-old woman who was admitted with an acute gastric outlet obstruction, requiring surgical intervention.
Surprisingly the “bezoar” turned out to be an impacted gallstone in the duodenum, creating a gastric outlet obstruction with a large cholecystoduodenal fistula.
Bouveret syndrome was first described in 1896 by French physician Leon Bouveret, and there were about 100 cases reported since then. To our knowledge our patient seems to be the oldest one.
Diagnosis of gallstone ileus based on Rigler’s triad includes bowel obstruction, pneumobilia, and an ectopic gallstone [6]. Our patient revealed air in the biliary tree and partial gastric outlet obstruction (according to abdominal plain film and gastrograffin swallow).
The majority of patients are elderly with associated medical comorbidities, thus initial preoperative therapy should include proximal decompression with a nasogastric tube, fluid resuscitation, and correction of electrolyte disturbances, to optimize the pre-operative condition. As a first step, a trial of endoscopic retrieval of the impacted stones in the gastric outlet zone should be encouraged to alleviate the blockage. When EGD fails, abdominal exploration should be carried out. The exploration is through a midline laparotomy, so that the entire small bowel, including the duodenum and the stomach could be inspected upon exploration, as well as the CBD, as multiple intraenteric stones may be present. Once the stones were identified, their extraction through the divided cholecystoduodenal fistula should be accomplished.
We believe that when a Bouveret syndrome is encountered, even in elderly patients, one should consider the surgical intervention as a viable option, if EGD extraction fails.
If surgery is selected, a well-trained surgical team should handle this rare and complicated case [7] after informing the patient and it’s family about all the possible complications.
CONCLUSIONS
Bouveret syndrome is a rare cause of gastric outlet obstruction in the elderly. There should be a high index of suspicion for high duodenal gallstone blockade in elderly patients with a previous history of gallstone disease. Use of abdominal CT scan is helpful in diagnosis of the obstructing lesion. Endoscopic treatment should be attempted. Surgery is an alternative option for treatment of impacted stone in the duodenum, when endoscopic option fails.
REFERENCES
- Artioli G, Muri M, Praticò FE, Marcantoni EA, Gazzani SE, et al. Gallstone ileus: literature review. Acta Biomed 2016; 87: 40-44. Ref.: https://goo.gl/UhDzKy
- Giese A, Zieren J, Winnekendonk G, Henning BF. Development of a duodenal gallstone ileus with gastric outlet obstruction (Bouveret syndrome) four months after successful treatment of symptomatic gallstone disease with cholecystitis and cholangitis: a case report. J Med Case Rep. 2010; 4: 376. Ref.: https://goo.gl/URhdsQ
- Yong E, Chiu TF, Kamel H, Yong E. To leave no stone unturned: cholelithiasis and subsequent gallstone ileus. BMJ Case Rep. 2016. Ref.: https://goo.gl/r4rTr0
- Mumoli N, Cei M, Luschi R, Carmignani G, Orlandi F. Bouveret syndrome. Emerg Med J. 2010; 277: 525. Ref.: https://goo.gl/SjholH
- Rossi D, Khan U, McNatt S, Vaughan R. Bouveret syndrome: a case report. W V Med J. 2010; 106: 18-22. Ref.: https://goo.gl/71s2Zs
- Gavrila D, Galusca C, Berbecel M, Boros M, Dumitrascu T. Bouveret Syndrome - An Exceptional Complication of a Very Frequent Disease. Chirurgia (Bucur). 2016; 111: 283-285. Ref.: https://goo.gl/n7Ixtq
- Vidal O, Seco JL, Alvarez A, Triñanes JP, Serrano LP, et al. Bouveret syndrome: 5 cases. Rev Esp Enferm Dig. 1994; 86: 839-844. Ref.: https://goo.gl/hTVgzd