
More Information
Submitted: 19 February 2020 | Approved: 20 July 2020 | Published: 21 July 2020
How to cite this article: Nurdağ A, Ceylan KC, Kaya SO. When conservative treatment in trachea laserations? Arch Surg Clin Res. 2020; 4: 022-023.
DOI: 10.29328/journal.ascr.1001047
ORCiD: orcid.org/0000-0003-0173-317X
Copyright License: © Nurdağ A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

When conservative treatment in trachea laserations?
Ahmet Nurdağ, Kenan Can Ceylan* and Şeyda Örs Kaya
University of Heath Sciences, Department of Thoracic Surgery, Dr. Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital, Turkey
*Address for Correspondence: Kenan Can Ceylan, M.D. University of Heath Sciences, Department Of Thoracic Surgery, Dr. Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital. Turkey, Tel: 00905053495446; Email: [email protected]
Introduction: The tracheobronchial injuries are usually fatal and some of the lucky people can reach emergency services without dying in the place of trauma. They can cause severe symptoms which can be lifetreathing. This type of injuries must been taken carefully and need to decide fast what treatment you going to give.
Case report: We present a 53 years old patient who has been stabbed during a fight and got his trachea ruptured. His complaints shortness of breath and neck swelling. He can be treated conservatively with bronchoscopic and clinical evaluation.
Discussion: Tracheobronchial injuries are life-threatening and the airway must be secured first. They can be treated conservatively in some cases. CT can be useful but fiberoptic bronchoscopy is the key in diagnosis.
Conclusion: Although early treatment of tracheal lacerations is urgent surgery, it is reported that these injuries can be treated with conservative methods under appropriate conditions.
Tracheobronchial injuries are rare and potentially life-threatening injuries due to their functions [1,2]. When the trauma cases that can reach the hospital emergency services are examined, it is seen that most of the cervical tracheal injuries are caused by penetrating injuries and most of the mediastinal tracheal injuries are caused by blunt injuries [3,4]. Trachealbronchial injuries may cause stridor, subcutaneous emphysema, severe respiratory distress, hemoptysis, hoarseness and pneumomediastinum [1,2]. In this case report we presenting a patient who has admitted to our emergency clinic with penetrating trauma to the trachea which we choose to treat him conservatively.
A 53-years old male patient was admitted to our emergency clinic with complaints of shortness of breath and neck swelling after a sharp stab wound. On physical examination, subcutaneous emphysema was palpated around both clavicle and approximately 2 cm incision was seen on the left side of the maneuver sterni (Photo 1).We sutured the patients wound and bandaged. Patients vital signs were within normal limits and his oxygen saturation was normal with nasal oxygen supplementation. There was pneumomediastinum and subcutaneous emphysema on his chest x-ray and he had no respiratory distress. After discussing the first results we decided to treat him conservatively. We followed his vital signs closely. After 4 hours we evaluate the patient with a new chest x-ray and there was no increase of pneumomediastinum and subcutaneous emphysema. His vital signs were stable and we decided to take a CT scan.
CT scan showed the fistula tract of the trauma which was in the left ending of membranous trachea and pneumomediastinum (Figure 1). We transferred the patient from emergency service to our clinic and continued to following him with nasal o2 supplementation. After 2 days nothing got worse on his medical condition, his subcutaneous emphysema were started to regress. We decided to do a flexible bronchoscopy.
With the flexible bronchoscopy we observed a rupture line has an active air inlet which was approximately 0.5 cm (Photo 2). The rupture had no air leakege anymore and started to heal.
After 4 days of clinical observation and medical symptomatic treatment the patients complaints and subcutaneous emphysema were regressed. He has no longer need for oxygen .On the control thorax CT, we can no longer see the fistula tract, pneumomediastinum and subcutaneous emphysema were receded. We did a flexible bronchoscopy and the rupture was totally healed by itself.
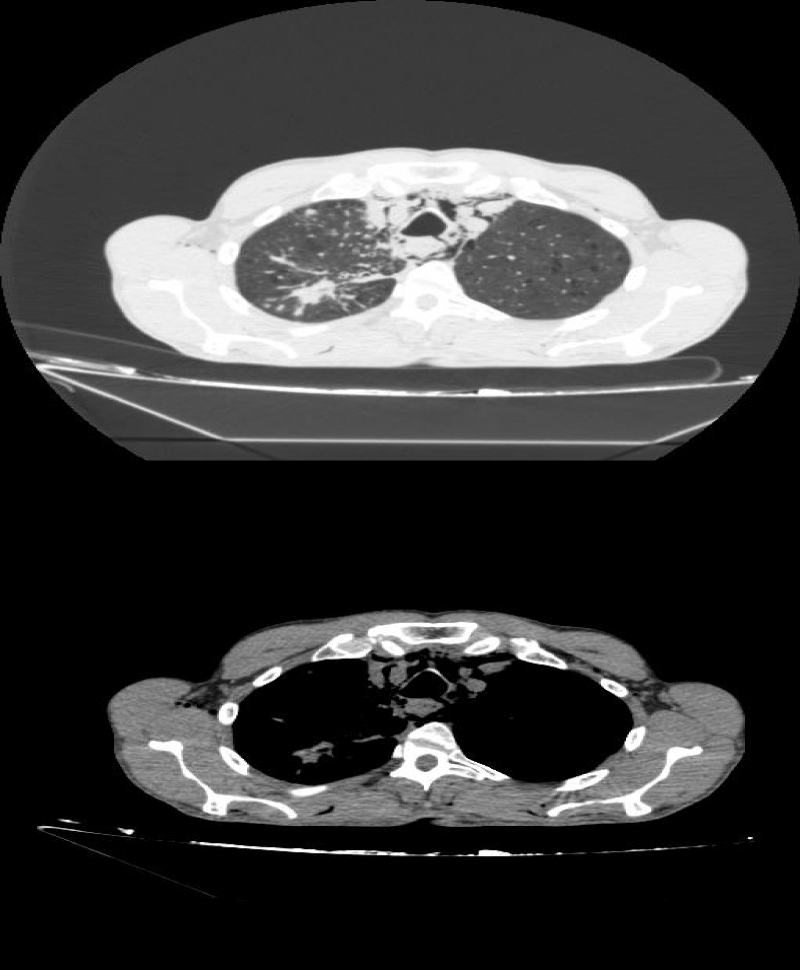
Figure 1:
Tracheobronchial injuries are life-threatening and should be decided fast for the treatment. In these patients, the airway safety must be provided firstly. For the airway safety, intubation can be perform with fiberoptic bronchoscopy or can be perform through laceration. After securing the airway, intracranial hemorrhages, major cardiovascular injuries and esophageal injuries should be determined first [5-7].
The definitive diagnosis of tracheobronchial injury is made by bronchoscopy. Improvements on computed tomography did not eliminate the necessity of bronchoscopy. Pneumomediastinum, refractory pneumothorax, air leakage to chest tube, marked subcutaneous emphysema, presence of atelectasis are indications for bronchoscopy [7].
For the patients who has uncomplicated mechanical ventilation without any loss of tidal volume, small laceration (supplemented with esophagus), subcutaneous emphysema not increased with moderate ventilation, tears less than 2 cm, or tears below 1/3 of the airway diameter (must not be with esophageal injury or mediastinitis, must no need for positive pressure ventilation and lung expansion can be provided with the chest tube which has regressing and disappearing air leakage on follow up or if there is no air leakage on first placement, conservative treatment can be applied [3,5,8,9].
The vital values of our patient in the evaluation of the emergency room were normal, there was only pneumomediastenium and fistula tract of the penetrating travma in CT scan. A 0.5 cm rupture line was observed in the bronchoscopic examination and the patient was followed with oxygen inhalation. After 3 days of clinical internation control
CT scan and bronchoscopy showed us the regression of tracheal laseration and the patient extenuated with no problem at all.
Although early treatment of tracheal lacerations is urgent surgery, they can be treated conservatively with bronchoscopic and clinical evaluation.it is reported that these injuries can be treated with conservative methods under appropriate conditions. In some publications, conservative treatment may be preferred in patients with tracheal lacerations smaller than 2 cm and stable clinical conditions.
- Carretta A, Melloni G, Bandiera A, Negri G, Voci C, et al. Conservative and surgical treatment of acute posttraumatic tracheobronchial injuries. World J Surg. 2011; 35: 2568-2574. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/21901327
- Gómez-Caro A, Ausin P, Moradiellos FJ, Díaz-Hellín V, Larrú E, et al. Role of conservative medical management of tracheobronchial injuries. J Trauma 2006; 61: 1426-1434. PubMed: https://pubmed.ncbi.nlm.nih.gov/17159686/
- Kieser AC, O’Brien SM, Detterbeck FC. Blunt Tracheobronchial Injuries: Treatment and Outcomes, Ann Thorac Surg. 2001; 71: 2059-2065. PubMed: https://pubmed.ncbi.nlm.nih.gov/11426809/
- Hahn B. Tracheabronchial Rupture. J Emerg Med. 2007; 33: 193-194. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/17692774
- Özdülger A. Trakeobronşiyal yaralanmalar. TTD Toraks Cerrahisi Bülteni. 2010; 1: 45-54.
- Baumgartner D, Sheppard B, de Virgilio C, Esrig B, Harrier D, et al. Tracheal and main bronchial disruptions after blunt chest trauma: Presentation and management. Ann Thorac Surg 1990; 50: 569-574. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/2222045
- Balcı AE. Trakeobronşiyal Yaralanmalar. Türkiye Klinikleri J Surg Med Sci. 2007; 3: 52-62.
- Koletsiz E, Prokakis C, Baltayiannis N, Apostolakis E, Chatzimichalis A, et al. Sugical decision making in tracheobronchial injuries on the basis of clinical evidences and injury’s anatomical setting: A Retrospective Analysis Injury. 2012; 43: 1437-4141. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20863493
- Schneider T, Konstantina S, Dienemann H. Management pf Iatrogenic Tracheobronchial Injuries: A Retrospective Analysis pf 29 Cases. Ann Thorac Surg. 2007; 83: 1960-1964. PubMed: https://pubmed.ncbi.nlm.nih.gov/17532378/