
More Information
Submitted: March 17, 2021 | Approved: April 01, 2021 | Published: April 02, 2021
How to cite this article: Shytaj S, Bottai V, Cosseddu F, Cifali R, De Franco S, et al. Michelangelo Scaglione. Bilateral transient osteoporosis of the hip with unilateral fracture in a 40 years old pregnant woman. Arch Surg Clin Res. 2021; 5: 007-010.
DOI: 10.29328/journal.ascr.1001058
ORCiD: orcid.org/0000-0001-7928-3186
Copyright License: © Shytaj S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Bilateral transient osteoporosis of the hip with unilateral fracture in a 40 years old pregnant woman
Sheila Shytaj*, Vanna Bottai, Fabio Cosseddu, Roberta Cifali, Silvia De Franco and Michelangelo Scaglione
Clinica Ortopedica e Traumatologica, Azienda Ospedaliera Universitaria Pisana, Pisa, Italy
*Address for Correspondence: Sheila Shytaj, Clinica Ortopedica e Traumatologica, Azienda Ospedaliera Universitaria Pisana, Via Paradisa 2 56124 Pisa, Italy, Tel: 0039050992025; Email: [email protected]
Purpose: Some physiological events in women’s life such as pregnancy and lactation can be associated to a condition known as Transient Osteoporosis of the Hip (TOH); if not promptly diagnosed it can lead to significant consequences such as femoral neck fracture. In this paper we describe a case of bilateral TOH, focusing on the importance of early treatment and how it influenced the outcome.
Methods: A 40 years old post-delivery woman came to our attention for hip pain and a left femoral neck fracture was diagnosed. Magnetic resonance (MRI) showed bilateral edema of the femoral head. She underwent total hip replacement on the left side; toe-touch weight bearing and pharmacological therapy were prescribed for the right hip.
Results: MRI at nine months showed complete regression of the femoral head and neck edema; the patient was clinically asymptomatic.
Conclusion: If not promptly diagnosed and treated, TOH can potentially evolve in fracture. Many therapeutic strategies have been suggested since now; we believe that avoiding weight bearing on the involved hip as early as possible is the key to recovery.
Bone tissue homeostasis relies on a fine balance that can be subjected to several variations during lifetime. A skeletal condition characterized by reduction of bone mass and alteration of bone architecture resulting in increased bone fragility and increased fracture risk, known as osteoporosis, is a common metabolic disease leading often to a vulnerability to fracture [1]. Osteoporosis is defined by the World Health Organisation (WHO) as a bone density 2.5 standard deviation below the mean value in young reference population measured through dual-energy X-ray absorptiometry (DEXA) [2]. Bone tissue is mainly composed of inorganic minerals, organic materials, cells, and adipose tissue. The mineral component providing stiffness to the collagenous fibres is hydroxyapatite, a Calcium-Phosphate hexagonal crystal that deposits by a process called crystallization. Adequate deposits of calcium are crucial for this process, which is also regulated by several hormonal influences [3, 4]. Bone density decrease is a typical condition of the elderly, however it can appear also in young patients under particular conditions, such as pregnancy. During gestation, several physiological adaptations are required in order to supply an amount of calcium and vitamin D to the fetus. These changes alter serum calcium and calciotropic hormones, however their values remain usually normal and clinically asymptomatic with fragility fractures occurring rarely [5]. However, a small percent of women develop clinically relevant symptoms. Kovacs [6] has identified three main clinical presentations of osteoporosis in the setting of recent pregnancy: osteoporosis, vertebral fractures and transient osteoporosis of the hip (TOH). The latter is a rare, self-limiting disease consisting in focal and transient osteoporosis of the hip associated to pain occurring in one or both hips with uncertain aetiology. We report a case of bilateral TOH in a 40 years old post-partum woman with femoral neck fracture.
Our patient, a 40 years old primiparous healthy woman, started to feel discomfort in her left hip about three months before delivery, without any level of trauma. She addressed to her gynaecologist who suggested the use of crutches for walking. She declined radiography because of concerns about dangers of ionising radiations. Until that moment, the pregnancy course had been regular, without any complication, except for slight arterial hypertension in the last month. Before getting pregnant, she underwent four intra-uterine inseminations and one in vitro fertilization as fertility treatment. She did not employ any kind of drugs during pregnancy. She had a vaginal delivery complicated by a postpartum haemorrhage that required blood transfusion. A week after her childbirth, she felt a pain flare in her left hip so she came to the emergency department of our hospital. She did not report contralateral groin pain. The patient had no preceding history of trauma, fever, metabolic disorders, smoking or alcohol abuse. The radiograph performed showed left femoral neck fracture (Figure 1). She soon underwent a magnetic resonance imaging (MRI) that excluded any oncological feature or other primary causes for the fracture; the MRI reported diffused marrow edema involving both femoral heads, which is a specific imaging finding of transient osteoporosis of the hip (Figure 2). A CT scan with three-dimensional reconstruction was also performed (Figure 3). All the routine laboratory tests for autoimmune and rheumatoid disease and those to detect osteoporosis (LAC, ACLA, protein electrophoresis, complete blood count, 24 hour excretion of calcium and creatinine, serum level of calcium, albumin, phosphorus, vitamin D, alkaline phosphatase, blood urea nitrogen and creatinine) resulted normal. Thyroid function, electrolytes and renal function tests were also in the range. A slight positivity to some tumoral markers (CA125, alpha-fetoprotein and ferritin) was detect and, after performing an abdominal ultrasound that excluded any kind of lesion, the gynaecologist explained the values as result of the recent pregnancy. Therefore, the case was managed operatively with total hip arthroplasty on the left side (Figure 4). The histopathological examination of the femoral head showed diffuse edema, but no signs of neoplastic proliferation or other pathological bone condition. Two days later, she performed a bone densitometry showing -1.6 for T-score value and -1.5 for Z-score value at the right femoral neck (Table 1). After that, she started a therapy with risedronate, vitamin D and calcium (risedronate 35 mg/week, calcium carbonate 500 mg/die, cholecalciferol 100000 UI/month). Considering that the edema involved also the right hip, a toe touch weight bearing on the lower right limb was prescribed, too. Two months later, she performed a new MRI that showed slight increase of the edema on the right marrow femoral head; clinically she felt still discomfort on her right hip. There were no significant clinical or radiographic findings regarding the left hip prosthesis and femur. She continued the same therapy for other six months, avoiding weight bearing on the right limb. After nine months from delivery, she performed a further MRI that reported an almost total regression of the edema (Figure 5). Moreover, at the clinical evaluation the patient did not report any pain or discomfort on both hips, so she was allowed to dismiss crutches and walk with full weight bearing. At the last clinical follow up at one year no complications raised: the patient walked independently without pain, with an almost full range of movement on both hips, able to manage a normal lifestyle.

Figure 1: Radiograph performed at the Emergency Department showing left femoral neck fracture.
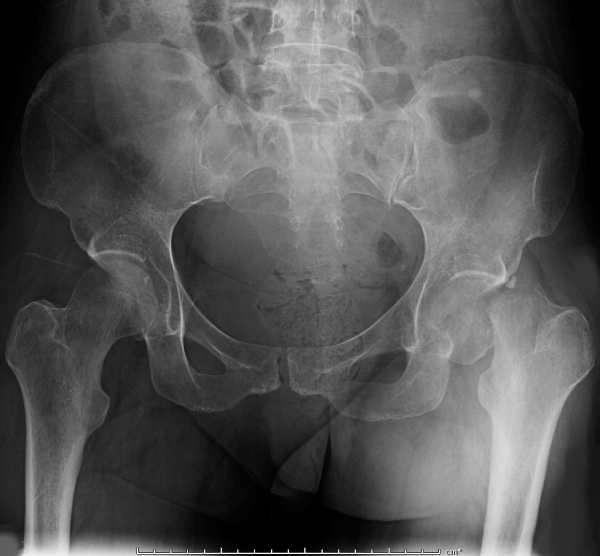
Figure 2: Magnetic Resonance showing diffused marrow edema involving both femoral heads.
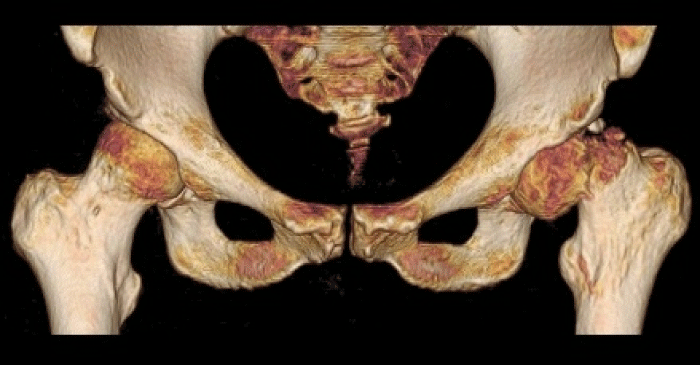
Figure 3: Three-dimensional reconstruction of the CT scan.
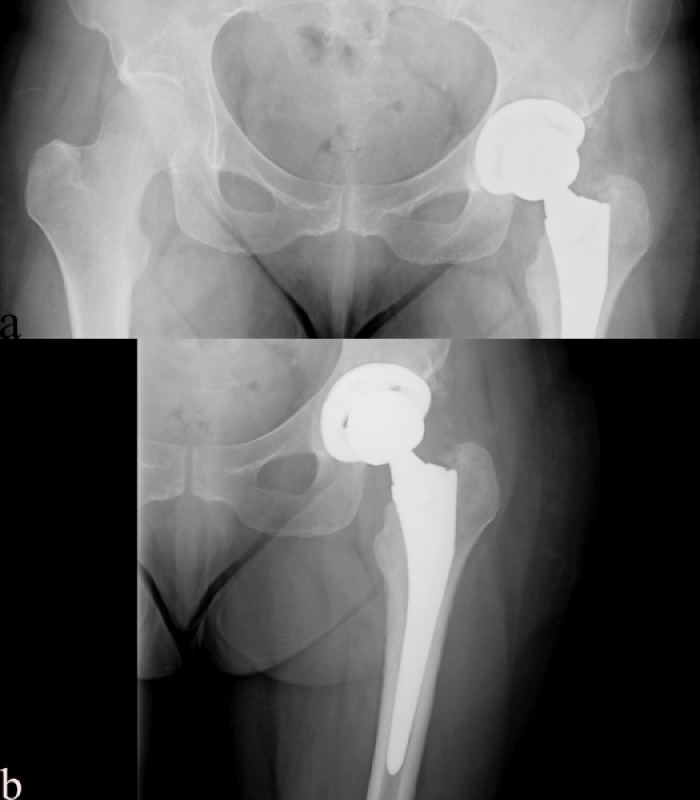
Figure 4: Post-operative radiograph, a (pelvis) b (left hip).

Figure 5: Magnetic resonance at nine months follow up showing edema regression.
| Table 1: First Densitometry. | |||
| BMD | T-score | Z-score | |
| Femoral neck | 0.782 | -1.6 | -1.5 |
| Total femur | 0.760 | -2.0 | -2.0 |
| L1-L4 | 0.941 | -2.0 | -2.0 |
| BMD: Bone Mineral Density at right (contralateral) femoral neck. | |||
During pregnancy and puerperium several alterations of skeletal turnover occur, particularly during the third trimester and lactation when it is reported a 3% to 10% loss of trabecular bone; usually these changes physiologically return soon to normality with restoration to the previous bone density in 6-12 months after weaning [5,6]. However, a few women experience fragility fracture during these times, even if it is an uncommon event. Kovacs, et al. [6] identified three clinical patterns of presentation of fragility fractures in the setting of recent pregnancy: vertebral fractures, generalized osteoporosis and transient osteoporosis of the hip (TOH). Vertebral fractures seems to be associated to an increased weight bearing and lordotic posture in women with prior risk factors, such as systemic osteoporosis, therapies with glucocorticoids, eating disorders [7]. As regards systemic osteoporosis, it can result from excessive bone resorption and impairment of restoration mechanisms. The third pattern identified by Kovacs is TOH, described as a rare and localized disorder of the hip not related to calciotropic hormones levels alterations [6]. The first report of TOH dates back to 1959 when Curtiss and Kincaid [8] performed an X-ray on three pregnant women suffering from hip pain and observed a radiolucent aspect of femoral head and neck. Following studies included this condition in the group of the primary bone edema syndromes (BMES) describing it as a self-limiting phenomenon, with uncertain etiology involving both males and females; for women the most common reported risk factor was pregnancy [9]. The aetiology of this condition remains still unclear. Presumably, the process of bone loss is initiated by an aspecific insult (eg injury, drugs abuse, infection) that leads to a local bone increased turnover with venous hypertension and edema. Patel, [10] has described a hypothetical aetiological pathway common to all bone marrow edema syndromes suggesting if these conditions can be considered as an early stage of osteonecrosis. If it is assumed so, an early and appropriate conservative treatment is mandatory in order to avoid the progression of the edema to an irreversible condition. The peculiarity of TOH is that it seems not related to systemic osteoporosis and does not feature changes in bone turnover markers. Moreover, it usually proceeds to gradual restoration without sequelae, discriminating it from other conditions in which edema progress to irreversible vascular compression may induce avascular necrosis of femoral head [10,11]. In our case, the patient developed bilateral TOH with femoral neck fracture occurring on the left side, where she was symptomatic during the last trimester of pregnancy; the pain in the controlateral hip begun after childbirth and was early diagnosed and treated. Currently, literature data do not report hip fracture incidence in TOH and whether there is a relation between the time of symptoms onset and fracture incidence. The diagnostic gold standard is MRI and the typical finding is bone marrow edema, sometimes bilateral as in our case. Some authors describe also a relation between the extent of edema at MRI and the time of recovery [12,13]. As regards our patient, the total clinical and radiological recovery was about nine months after the onset of right hip pain. Being MRI a harmless diagnostic tool for both child and mother, we suggest to perform it as soon as the suspect for a TOH arises, in order to have an early diagnosis and reduce possible complications such as fracture or progression to avascular necrosis. Bone mineral density (BMD) detected with densitometry showed diffused osteopenia and it is accordant to literature data [14]. As regards treatment, there is actually no consensus: of course restricted weight bearing, physiotherapy, analgesics and thromboprophylaxis are crucial, especially during pregnancy, also considering the risk of placenta cross for several drugs. However, some authors report good results, consisting in a quicker recovery time, with the use of biphosphonates, calcitonin, teriparatide or combinations of these drugs. Biphosphonates have a well-known antiresorptive effect however are controindicated during pregnancy for their potential effects on fetal development; injectable calcitonin appears safe and may reduce recovery time; teriparatide is a good bone promoting agent with a lifetime duration of 18 to 24 months, so some authors suggest to avoid it during reproductive years [6,9]. Some authors on the other hand suggest to consider that bone density normally increases during the 6 to 12 months after weaning, reconsidering the real efficacy of pharmacological treatment [6]. Our patient was treated with risedronate, Calcium and Vit. D interrupting breast-feeding; restricted weight bearing on the right side and rest were part of the treatment, too. Basing on our experience and literature data, we believe that weight bearing restriction actually prevented our patient from a bilateral fracture, even more than pharmacological therapy. The clinical recovery at nine months was satisfactory, as confirmed also by MRI.
The purpose of our paper is to increase the attention towards hip pain in pregnant women, underlining the important role of general physician and gynaecologist, which are the closest figure to the patient. The clinical suspect should lead to a prompt diagnosis and personalized early treatment, avoiding weight bearing and thus minimizing the risk of fracture, which is an undesirable event especially during pregnancy. Nevertheless, we believe that further investigations are required to determine the incidence of fracture in TOH and the real efficacy of pharmacological treatment.
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work.
A case of transient osteoporosis of the hip with fracture during pregnancy.
- Akkawi I, Zmerly H. Osteoporosis: Current Concepts. Joints. 2018; 6: 122–127. PubMed: https://pubmed.ncbi.nlm.nih.gov/30051110/
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. Geneva, World Health Organization. 1994. 843; 1-129. PubMed: https://pubmed.ncbi.nlm.nih.gov/7941614/
- Li L, Wang Z. Ovarian Aging and Osteoporosis. Adv Exp Med Biol. 2018; 1086: 199–215. PubMed: https://pubmed.ncbi.nlm.nih.gov/30232761/
- Cano A, Chedraui P, Goulis DG, Lopes P, Mishra G, et al. Calcium in the prevention of postmenopausal osteoporosis: EMAS clinical guide. Maturitas. 2018; 107: 7–12. PubMed: https://pubmed.ncbi.nlm.nih.gov/29169584/
- Kovacs CS. Calcium and bone metabolism disorders during pregnancy and lactation. Endocrinol Metab Clin North Am. 2011; 40: 795–826. PubMed: https://pubmed.ncbi.nlm.nih.gov/22108281/
- Kovacs CS, Ralston SH. Presentation and management of osteoporosis presenting in association with pregnancy or lactation. Osteoporos Int. 26: 2223–2241. PubMed: https://pubmed.ncbi.nlm.nih.gov/25939309/
- Raffaetà G, Mazzantini M, Menconi A, Bottai V, Falossi F, et al. Osteoporosis with vertebral fractures associated with pregnancy: two case reports. Clin Cases Miner Bone Metab. 2014; 11: 136–138. PubMed: https://pubmed.ncbi.nlm.nih.gov/25285145/
- Curtiss PH Jr, Kincaid WE. Transitory demineralization of the hip in pregnancy. A report of three cases. J Bone Joint Surg Am. 1959; 41-A: 1327–1333. PubMed: https://pubmed.ncbi.nlm.nih.gov/13849487/
- Asadipooya K, Graves L, Greene LW. Transient osteoporosis of the hip: review of the literature. Osteoporos Int. 2017; 28: 1805–1816. PubMed: https://pubmed.ncbi.nlm.nih.gov/28314897/
- Patel S. Primary bone marrow oedema syndromes. Rheumatology (Oxford). 2014; 53: 785–792. PubMed: https://pubmed.ncbi.nlm.nih.gov/24080251/
- Balakrishnan A, Schemitsch EH, Pearce D, McKee MD. Distinguishing transient osteoporosis of the hip from avascular necrosis. Can J Surg. 2003; 46: 187–192. PubMed: https://pubmed.ncbi.nlm.nih.gov/12812240/
- Malizos KN, Zibis AH, Dailiana Z, Hantes M, Karachalios T, et al. MR imaging findings in transient osteoporosis of the hip. Eur J Radiol. 2004; 50: 238–244. PubMed: https://pubmed.ncbi.nlm.nih.gov/15145483/
- Ergun T, Lakadamyali H. The relationship between MRI findings and duration of symptoms in transient osteoporosis of the hip. Acta Orthop Traumatol Turc. 2008; 42: 10–15. PubMed: https://pubmed.ncbi.nlm.nih.gov/18354271/
- Anai T, Urata K, Mori A, Miyazaki F, Okamoto S. Transient osteoporosis of the hip in pregnancy associated with generalized low bone mineral density—a case report. Gynecol Obstet Investig. 2013; 76: 133–138. PubMed: https://pubmed.ncbi.nlm.nih.gov/23796944/