
More Information
Submitted: February 10, 2026 | Accepted: February 23, 2026 | Published: February 24, 2026
Citation: Islam SR, Sarkar SA, Poran S. Emergency Altemeier’s Operation for Strangulated Rectal Prolapse: A Case Report. Arch Surg Clin Res. 2026; 10(1): 001-003. Available from:
https://dx.doi.org/10.29328/journal.ascr.1001094.
DOI: 10.29328/journal.ascr.1001094
Copyright license: © 2026 Islam SR, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Rectal prolapse; Strangulation; Altemeier’s operation

Emergency Altemeier’s Operation for Strangulated Rectal Prolapse: A Case Report
Sardar Rezaul Islam1, Shah Alam Sarkar2 and Shah Poran3
1Professor and Head, Department of Surgery, Ad-din Women’s Medical College Hospital (AWMCH), Dhaka, Bangladesh
2Associate Professor, Department of Surgery, AWMCH, Dhaka, Bangladesh
3Assistant Professor, Department of Surgery, JIMCH, Bangladesh
*Corresponding author: Sardar Rezaul Islam, Professor and Head, Department of Surgery, Ad-din Women’s Medical College Hospital (AWMCH), Dhaka, Bangladesh, Email: [email protected]
Introduction: Rectal prolapse is defined as the protrusion of the rectal wall through the anal canal. Most rectal prolapses are reduced spontaneously, or the patient can reduce them manually. On rare occasions, the prolapsed segment cannot be reduced, leading to secondary complications like incarceration and strangulation. Emergency surgical intervention becomes mandatory when an ischemic complication occurs.
Case report: We report a case of a 45-year-old male who presented with a painful and irreducible rectal prolapse. The prolapsed rectum was large, incarcerated, and the mucosa looked gangrenous. Emergency surgery was performed using Altemeier’s procedure. This surgical procedure consists of total resection of the prolapsed rectum and colon. Then colo-anal anastomosis was done in the same sitting. A covering loop sigmoid colostomy was done to ensure the uncomplicated healing of edematous bowel. Sigmoid colostomy was closed 3 months after the procedure. The bowel continuity was confirmed by barium enema before closure of colostomy. This case illustrates the successful management of a challenging case of rectal prolapse with gangrene of bowel.
Rectal prolapse is defined as the protrusion of the rectal wall through the anal canal. There are three types of rectal prolapse. These are full-thickness rectal prolapse, mucosal prolapse, and internal rectal prolapse. The first two types are visible outside the anal verge. The third type is characterized by the invagination of the rectum into the anal canal without extending beyond the anal verge. This type of rectal prolapse is associated with obstructed defecation syndrome (ODS).
Incidence of rectal prolapse in adults ranges from 2.5 to 4.2 per 100,000 people [1]. It is six to 10 times more common in women, especially those over 50 years of age, and in multiparous women [2]. Although it can occur at any age, it is more prevalent in childhood and the geriatric population. The pathophysiology of rectal prolapse is complex and multifactorial. Commonly associated risk factors include multiparity, a history of vaginal delivery or pelvic surgery, pelvic floor dysfunction, chronic constipation, diarrhea, or neurological diseases [3]. The diagnosis of rectal prolapse is primarily clinical, based on the history and physical examination. Complementary studies, such as colonoscopy, ultrasound, or magnetic resonance imaging, can rule out associated pathologies or predisposing conditions. Usually, rectal prolapse can be reduced spontaneously or with manual maneuvers; the irreducibility of the prolapsed segment can lead to severe complications such as pain, bleeding, strangulation, or perforation [4]. Surgery is the cornerstone of the management of rectal prolapse. Surgical techniques are grouped into abdominal and perineal approaches.
In the abdominal approach, fixation is done with or without resection of the rectum. Rectum is suspended by a piece of mesh (Mesh rectopexy) or without mesh (Ripstein rectopexy). This has lower recurrence rates but carries higher postoperative morbidity [5]. Abdominal approach is reserved for conditions where a substantial degree of pelvic floor descent is present.
The perineal approach is reserved for elderly patients or those with comorbidities [6]. This approach has a low morbidity but a high recurrence rate. There are two popular procedures in the perineal approach, named Delorme’s procedure and Altemeier’s procedure. In Delorme’s procedure rectal mucosa is partially removed, and the rectal muscle layers are plicated. Rectum must be viable. In Altemier's procedure, all layers of the rectum are transected, and colo-anal anastomosis is done by hand-sewn or circular stapler. This procedure is very suitable when the viability of the prolapsed rectum is doubtful due to compromised blood supply [6]. Transanal resection of rectum (STARR operation) is done for internal rectal prolapse causing obstructed defecation syndrome or mucosal rectal prolapse. This is a bloodless operation where anterior and posterior resection of the rectum is done with the help of two circular staplers [7].
A 45-year-old man presented in the emergency department with a painful and irreducible rectal prolapse. Patient gave a history of recurrent rectal prolapse for 2 years. On examination, he was found in severe pain and discomfort, with a prolapsed rectum that looked swollen, congested with black discoloration of the mucosa (Figure 1). He experienced severe tenderness on the attempt of manual reduction. A decision was taken to perform emergency surgery. He was operated on within 6 hours of admission on the emergency list. Per-operatively, all layers of the prolapsed rectum were found unviable. Complete resection of the rectum and colon was done by Altemeier’s procedure. The rectum was transected 3 cm proximal to the dentate line. The circular stapler could not be used for colo-anal anastomosis as the rectal wall was severely edematous. Anastomosis was done by an interrupted Vicryl suture (Figure 2). The rectum was then pushed back to the pelvis easily (Figure 3). A transabdominal loop sigmoid colostomy was done to ensure uncomplicated healing of the edematous anastomosis. Sigmoid colostomy was closed 3 months after Altemeier’s procedure. The bowel continuity and good patency were confirmed by barium enema before closure of colostomy (Figure 4). Patient made an uneventful recovery after colostomy closure. His defecation was normal. There was no incontinence either. There was no recurrence of prolapse after one year follow up.

Figure 1: Gangrenous rectal prolapse.
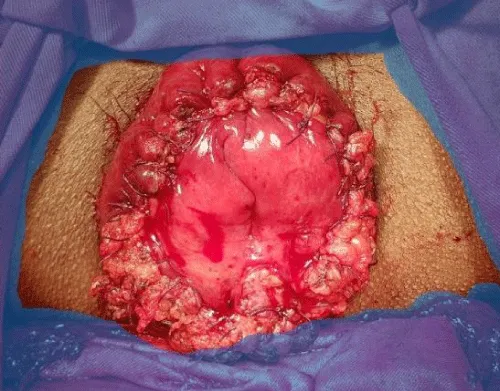
Figure 2: Colo-anal anastomosis with edematous bowel.
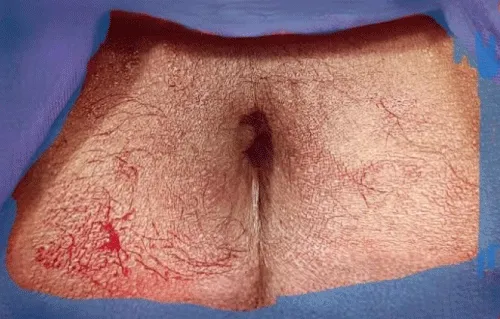
Figure 3: Prolapsed part is reduced.

Figure 4: Good lumen on Barium enema.
There are two surgical approaches for full-thickness rectal prolapse, which are the abdominal approach and the perineal approach. Our case was an incarcerated full-thickness prolapse of the rectum. Hence abdominal approach was not at all suitable. In this situation perineal approach was the only option. Due to gangrene of the rectum and sigmoid colon, complete resection of the prolapsed bowel and colo-anal anastomosis was necessary. Another name is Altemeier’s operation. Anastomosis of edematous bowel was a concern in our case. Fortunately, the anastomotic line was not ischemic but edematous only. Circular stapler-assisted anastomosis was not feasible for the same reason. A trans-abdominal construction of a sigmoid loop colostomy was needed to protect the hand-sewn anastomosis. A protecting loop ileostomy could also be an alternative. There are some case series of Altemeier’s operation where a loop ileostomy was performed with good results [3,8]. But if elective Altemeier’s operation is done after bowel preparation, a protective stoma is not necessary [9].
Delorme’s procedure is done for full-thickness prolapse, but with a viable rectum. In this procedure, muscle layers of the prolapsed rectum are plicated and shortened after partial degloving of the rectal mucosa. When the prolapsed rectum is incarcerated, Delorme’s procedure is not suitable for our patient. Altemeier’s operation (proctosigmoidectomy) becomes appropriate. In recent years, there has been a trend towards elective Altemeier’s operation in healthier young patients, especially in males. Altemeier’s seem to have less recurrence than Delorme’s procedure. Recurrence rate was found to be is 8% vs 16% in one study [10]. Preservation of continence following this operation is also unpredictable. The cause of increased frequency or incontinence is multifactorial. Reduction in the capacity of the rectum, dysfunction of the external sphincter complex, and pelvic floor dysfunction. Increased frequency of bowel movement usually improves over the period of time as the capacity of the rectum gradually increases.
Abdominal approaches are performed in patients who are fit enough to tolerate laparotomy or laparoscopy. There is a slight increased risk of impotence or infertility for young men in abdominal rectopexy [11,12]. Rectopexy is done using fixation material such as mesh, sutures, or clips. This is most popular technique with good results regarding recurrence [13]. The fixation with presacral fascia can be done either anteriorly (Ripstein) or posteriorly. However, when constipation is a dominant symptom, usually with associated redundant sigmoid, anterior resection with combination of rectopexy is usually preferred. In the modern era ventral rectopexy is performed by laparoscopy with less morbidity and mortality [14]. This operation gives good result when prolapse is associated with substantial degree of ano-rectal descent seen on MR defecography.
This is a rare situation of strangulated rectal prolapse with gangrenous bowel. Emergency Altemeier’s operation was very appropriate treatment for this patient with incarcerated rectum and sigmoid colon. This case also emphasizes importance of early surgical intervention in case of strangulated bowel. A protective loop colostomy helped achieve uncomplicated healing of colo-anal anastomosis. This case illustrates successful management of a challenging and uncommon presentation of rectal prolapse.
- Soni RC, Parmar KD, Parikh S, Khatri UK. Altemeier procedure for incarcerated rectal prolapse in young age: a rare case report. Int Surg J. 2024;11(7):1201-1203. Available from: https://www.ijsurgery.com/index.php/isj/article/view/10432
- Chaouch MA, Sallem R, Jabra SB, Chedly E, Gafsi B, Noomen F. Altemeier procedure for strangulated rectal prolapse: a case report. Int J Surg Case Rep. 2024;114:109216. Available from: https://doi.org/10.1016/j.ijscr.2023.109216
- Mantzoros I, Brenta A. Perineal rectosigmoidectomy (Altemeier’s procedure) in the treatment of strangulated rectal prolapse: a case series and literature review. J Pers Med. 2024;14(11):1095. Available from: https://doi.org/10.3390/jpm14111095
- Ahmadinejad M, Farsi Y, Bahr MH, Bozorgmehr R, Soltanian A, Zebarjadi Bagherpour J. A case report of largest rectal prolapse in the literature successfully treated with Altemeier’s procedure. Ann Med Surg. 2022;80:104231. Available from: https://doi.org/10.1016/j.amsu.2022.104231
- Khan AA, Cervera LF, Shihadeh S, Glotzer D. Large anal polyp disguised as rectal prolapse. Cureus. 2024;16:10.7759/cureus.65193. Available from: https://doi.org/10.7759/cureus.65193
- Pandya B, Golmei J, Henriques MS, Dawar A. To do or not to do: prolapsed, bleeding, rectal polyp, a dilemma in austere circumstances. J Surg Case Rep. 2020;2020:rjaa400. Available from: https://doi.org/10.1093/jscr/rjaa400
- Ripamonti L, Guttadauro A, Lo Bianco G, Rennis M, Maternini M, Cioffi G, et al. Stapled transanal rectal resection (STARR) in the treatment of obstructed defecation: a systematic review. Front Surg. 2022;9:790287. Available from: https://doi.org/10.3389/fsurg.2022.790287
- Roy HM, Baig Z, Karimuddin AA, Raval MJ, Brown CJ, Phang PT, et al. A comparison of perineal stapled prolapse resection and the Altemeier’s procedure at 2 Canadian academic hospitals. Can J Surg. 2023 Jan 3. Available from: https://doi.org/10.1503/cjs.008421
- Khalil MI, Alam ABMK, Jahan SK, Saleh AZ. Altemeier’s procedure, an easy solution for rectal prolapse. J Bangladesh Coll Physicians Surg. 2022 Oct;40:229-232. Available from: https://www.banglajol.info/index.php/JBCPS/article/view/61878
- Bhattacharya P, Hussain MI, Zaman S, Randle S. Delorme's vs. Altemeier's in the management of rectal procidentia: systematic review and meta-analysis. Langenbecks Arch Surg. 2023 Dec 2;408(1):454. Available from: https://doi.org/10.1007/s00423-023-03181-z
- Libânio D, Meireles C, Afonso LP, Henrique R, Pimentel-Nunes P, Dinis-Ribeiro M. Mucosal prolapse polyp mimicking rectal malignancy: a case report. GE Port J Gastroenterol. 2016;23:214-217. Available from: https://doi.org/10.1016/j.jpge.2015.12.009
- Munteanu I, Mihaela M, Popescu S, Slavu IM, Macovei AO, Cochior D. Giant villous adenoma of the rectum with prolapse: case report. Cureus. 2023;15:10.7759/cureus.50079. Available from: https://doi.org/10.7759/cureus.50079
- Cano-Contreras AD, Meixueiro-Daza A, Grube-Pagola P, Remes-Troche JM. Giant rectal polyp prolapse in an adult patient with the Peutz-Jeghers syndrome. BMJ Case Rep. 2016;2016:bcr-2016-215629. Available from: https://doi.org/10.1136/bcr-2016-215629
- Bordeianou L, Hicks CW, Kaiser AM, Alavi K, Sudan R, Wise PE. Rectal prolapse: an overview of clinical features, diagnosis, and patient-specific management strategies. J Gastrointest Surg. 2014;18:1059-1069. Available from: https://doi.org/10.1007/s11605-013-2427-7